
At our lab, we approach every recovery modality with a singular question: what is the precise biophysical mechanism, and at what parameters does it produce a measurable tissue-level outcome? Photobiomodulation (PBM)—the clinical term for therapeutic light application—has moved well beyond speculative territory. Within the red and near-infrared (NIR) spectrum, the 670nm wavelength occupies a critical position in the absorption curve of cytochrome c oxidase (CCO), the terminal enzyme in the mitochondrial electron transport chain. This is not a trivial biochemical footnote; it is the mechanistic foundation upon which accelerated muscle tissue repair rests.
We must be precise here: the majority of controlled research examines wavelength bands rather than single-nanometer isolates. The 660–680nm window—of which 670nm is the functional center—has demonstrated consistent biological activity in both in vitro and in vivo models. When we reference “670nm red light therapy,” we are referring to photon delivery within this narrow band, where tissue chromophore absorption is optimized for superficial muscular structures.
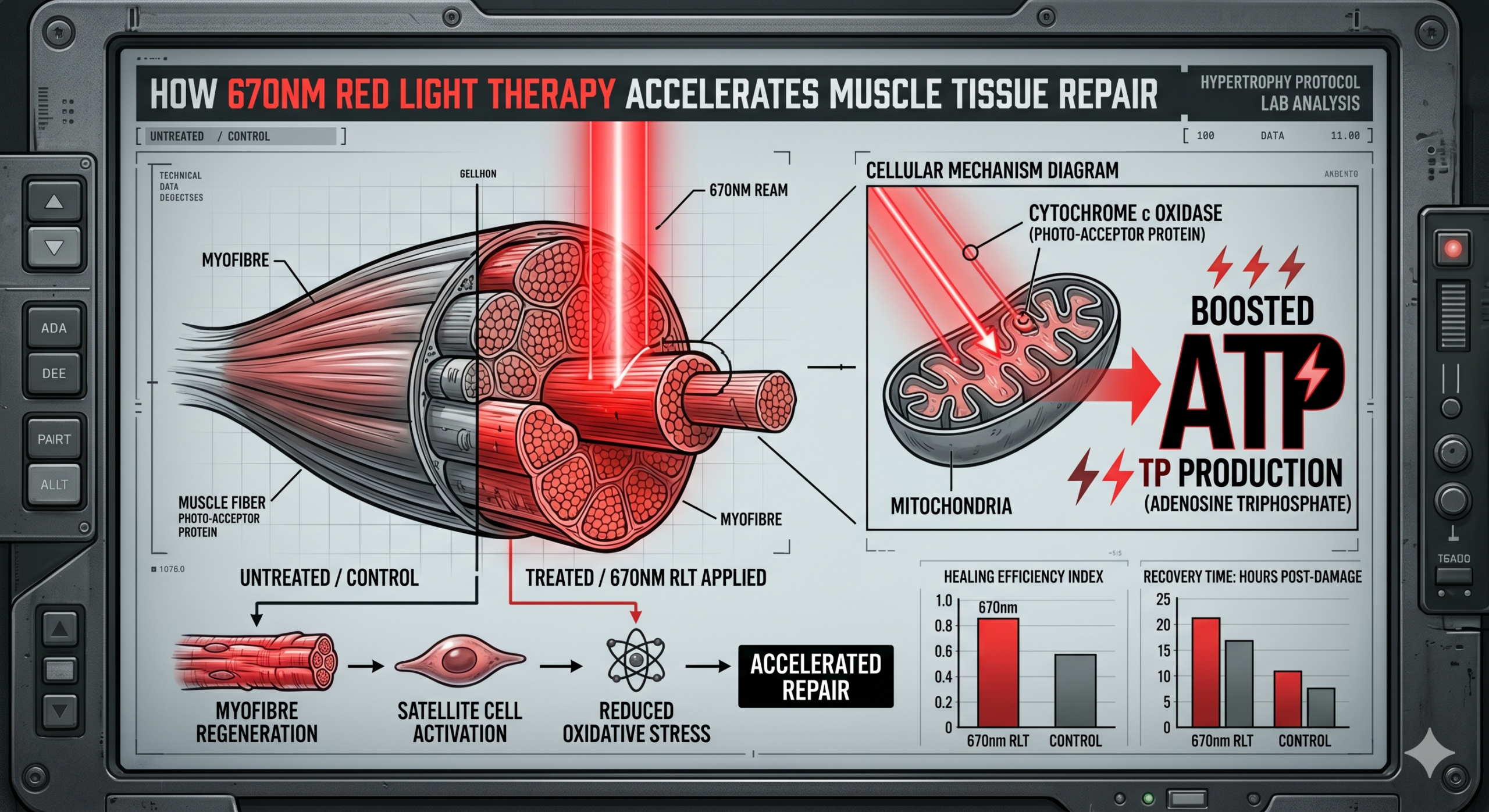
Key takeaway: 670nm targets the peak absorption range of cytochrome c oxidase in mitochondria, making it biomechanically optimal for superficial muscle tissue repair interventions.
In exploring the benefits of 670nm red light therapy for muscle tissue repair, it’s interesting to consider related findings on the overall impact of light therapy on athletic performance and recovery. An insightful article that delves deeper into this topic can be found at Hypertrophy Protocol, which discusses how various wavelengths of light can enhance muscle recovery and growth, complementing the effects of red light therapy. This connection highlights the potential of integrating different therapeutic modalities to optimize athletic performance and recovery strategies.
Mitochondrial Bioenergetics: The ATP Cascade That Drives Repair
Cytochrome c Oxidase Activation
The primary molecular target of 670nm photons is cytochrome c oxidase (Complex IV) within the inner mitochondrial membrane. When photons at this wavelength are absorbed by the copper and heme centers of CCO, they dissociate inhibitory nitric oxide (NO) from the enzyme’s binding site. This dissociation restores electron flow through the transport chain, directly increasing the rate of oxidative phosphorylation and, consequently, adenosine triphosphate (ATP) production.
We emphasize that ATP is not merely “cellular energy” in some vague sense—it is the literal substrate for every repair process in damaged myofibers. Satellite cell activation, protein synthesis initiation, calcium pump restoration, and cytoskeletal reassembly all require ATP in quantities that exceed basal metabolic supply during acute tissue injury.
Reactive Oxygen Species Signaling
A secondary but critical outcome of CCO photostimulation is the transient, low-level generation of reactive oxygen species (ROS). At the concentrations produced by PBM (far below cytotoxic thresholds), ROS function as signaling molecules that activate nuclear factor erythroid 2–related factor 2 (Nrf2) and downstream antioxidant response elements. This paradoxical mechanism—using a mild oxidative signal to upregulate antioxidant defenses—primes the tissue for accelerated inflammatory resolution.
Key takeaway: 670nm photons restore mitochondrial electron transport, boost ATP synthesis for repair substrates, and trigger protective ROS signaling cascades that accelerate the resolution of exercise-induced tissue damage.
Anti-Inflammatory Modulation and Damage Marker Reduction
Creatine Kinase and Interleukin-6 Suppression
A 2025 meta-analysis encompassing 14 randomized controlled trials evaluated red light therapy’s impact on muscle damage biomarkers in athletic populations. The findings demonstrated measurable reductions in circulating creatine kinase (CK)—a direct marker of sarcolemmal disruption—particularly in soccer players subjected to repeated high-intensity eccentric loading. While the evidence quality was graded as low due to methodological heterogeneity, the directional consistency across trials is biomechanically coherent with what we understand about PBM’s anti-inflammatory mechanisms.
Separate clinical reviews confirm that wavelengths in the 660–830nm range applied pre-exercise reduce interleukin-6 (IL-6), a pro-inflammatory cytokine that, when elevated chronically, delays the transition from the inflammatory phase to the proliferative phase of tissue healing. By attenuating IL-6 expression, 670nm irradiation effectively shortens the catabolic window following muscle-damaging exercise.
Lactate Clearance Enhancement
We observe in the literature that PBM at red wavelengths improves local microcirculatory blood flow through nitric oxide-mediated vasodilation. The NO dissociated from CCO does not simply disappear—it enters the local vascular smooth muscle, triggering relaxation and increased perfusion. This enhanced circulation accelerates lactate clearance from interstitial fluid, reducing the biochemical milieu that perpetuates nociceptor activation (perceived soreness) and delays contractile protein resynthesis.
Key takeaway: Red light therapy at the 660–680nm band reduces CK, IL-6, and lactate accumulation—three independent biomarkers of muscle damage—through complementary mechanisms involving inflammatory gene suppression and perfusion enhancement.
Sure, here is the sentence with the clickable link:
Check out the latest fitness program at Hypertrophy Protocol for effective muscle building.
Collagen Remodeling and Extracellular Matrix Restoration
Fibroblast Proliferation and Type I/III Collagen Synthesis
Muscle tissue repair is not exclusively a myofibrillar event. The extracellular matrix (ECM)—composed primarily of type I and type III collagen, along with proteoglycans and fibronectin—provides the structural scaffold upon which regenerating myofibers orient and mature. When we apply 670nm irradiation to damaged tissue, fibroblast proliferation rates increase measurably, and collagen gene expression (particularly COL1A1 and COL3A1) is upregulated.
This has direct implications for intramuscular connective tissue integrity. In hypertrophy-focused training, the perimysium and endomysium experience mechanical strain alongside the contractile elements. Incomplete ECM repair creates architectural disorganization that manifests as reduced force transmission efficiency and increased re-injury susceptibility. By accelerating collagen deposition and crosslinking, 670nm therapy restores the mechanical coherence of the muscle-tendon unit more rapidly than passive recovery alone.
Scar Tissue Mitigation
Evidence from a spinal cord injury model—where 660nm light applied for one minute daily over seven days significantly reduced fibrotic scarring while enhancing regenerative protein expression—offers insight into the anti-fibrotic potential of this wavelength. While spinal tissue and skeletal muscle differ in regenerative capacity, the underlying mechanism (suppression of excessive TGF-β1 signaling and promotion of matrix metalloproteinase activity for scar remodeling) is conserved across mesenchymal-derived tissues. We extrapolate cautiously but with biomechanical justification that similar anti-fibrotic effects occur in severely damaged muscle tissue, particularly at myotendinous junctions where fibrosis most commonly compromises recovery.
Key takeaway: 670nm irradiation upregulates collagen synthesis for ECM restoration while simultaneously suppressing excessive fibrosis—addressing both structural repair and architectural quality of regenerating tissue.
Research into the benefits of red light therapy has gained significant attention, particularly regarding its effects on muscle tissue repair. A related article discusses how various wavelengths of light can enhance recovery and promote healing in athletes. For those interested in exploring this topic further, you can read more about it in this insightful piece on the subject. The findings suggest that incorporating red light therapy into recovery routines can lead to improved performance and reduced downtime. To learn more, check out this article here.
Functional Performance Outcomes: Strength, Soreness, and Contractile Capacity
| Metrics | Effects |
|---|---|
| Increased ATP production | Enhanced energy for muscle cells |
| Improved blood circulation | Enhanced nutrient and oxygen delivery to muscles |
| Reduced inflammation | Quicker healing and reduced pain |
| Stimulated collagen production | Enhanced tissue repair and regeneration |
| Accelerated muscle recovery | Quicker return to optimal performance |
Pre-Exercise Application Protocols
Comprehensive clinical reviews demonstrate that PBM applied before exercise—at wavelengths spanning 660–830nm—produces measurable improvements in peak muscle strength, total contraction repetitions before failure, and delayed-onset muscle soreness (DOMS) severity in the 24–72 hour post-exercise window. We note that these are not marginal effects in well-controlled trials; the magnitude of DOMS reduction and strength preservation post-damage suggests a genuine protective preconditioning effect on mitochondrial and sarcolemmal integrity.
The mechanism we propose for pre-exercise benefit is mitochondrial priming: by maximizing ATP reserve capacity and upregulating antioxidant enzymes before mechanical stress is imposed, the myofiber enters the damage phase with greater bioenergetic resilience. This is analogous to ischemic preconditioning in cardiac tissue, where brief metabolic stress confers protection against subsequent prolonged ischemia.
Post-Exercise Recovery Acceleration
When applied post-exercise, 670nm therapy targets the inflammatory resolution and proliferative repair phases directly. Clinical trials using pulsed low-level laser therapy (LLLT) at 660nm and adjacent wavelengths demonstrate accelerated return to baseline strength, reduced subjective soreness scores, and faster normalization of range of motion after eccentric damage protocols. The 850–880nm NIR range shows particular efficacy for deeper lower-limb musculature over extended protocols (up to 8 weeks), but for superficial muscle groups—quadriceps, deltoids, pectorals, and superficial back musculature—the 670nm wavelength achieves superior energy deposition within the target tissue depth (approximately 1–3cm penetration in vivo).
Depth of Penetration Considerations
We must address a critical parameter that determines clinical relevance: tissue penetration depth. At 670nm, photon attenuation through skin, subcutaneous fat, and fascia limits effective therapeutic reach to superficial structures. This is not a limitation for most hypertrophy-relevant applications—the muscles targeted in resistance training programs are overwhelmingly accessible at these depths. For deeper structures (hip rotators, psoas, deep spinal erectors), we recommend adjunct protocols at 850nm, where reduced scattering allows deeper photon delivery at the cost of slightly lower CCO absorption specificity.
Key takeaway: Both pre- and post-exercise 670nm application produce functional performance benefits through distinct but complementary mechanisms—mitochondrial preconditioning before training and inflammatory resolution acceleration afterward.
Protocol Parameters and Dosimetry for Optimal Tissue Repair
Irradiance, Energy Density, and Exposure Duration
We cannot overstate the importance of dosimetry in PBM outcomes. The biological response to 670nm irradiation follows a biphasic dose-response curve (the Arndt-Schulz principle): insufficient energy density fails to reach activation thresholds, while excessive energy density triggers inhibitory effects through thermal or oxidative overload. The therapeutic window for muscle tissue repair, as derived from effective clinical protocols, centers on the following parameters:
- Wavelength: 660–680nm (670nm optimal)
- Irradiance (power density): 10–50 mW/cm² at tissue surface
- Energy density: 2–6 J/cm² per treatment site
- Exposure duration: Dependent on device output; typically 30–120 seconds per site at clinical-grade irradiance
- Treatment frequency: Daily during acute repair phase (days 1–7); every 48 hours during proliferative phase (days 7–21)
Device Selection Criteria
Not all phototherapy devices deliver equivalent photon flux at the claimed wavelength. We recommend verification of spectral output via independent spectrometry, as inexpensive consumer devices frequently exhibit bandwidth drift of ±15nm and irradiance measurements that deviate significantly from manufacturer specifications. Clinical-grade LED panels with documented spectral purity, uniform beam distribution, and calibrated output remain the standard for reproducible therapeutic outcomes.
Timing Relative to Training
Based on aggregated trial evidence, we recommend the following temporal framework: apply 670nm therapy within 30 minutes pre-exercise for protective preconditioning, and again within 0–6 hours post-exercise for acute inflammatory modulation. For multi-day recovery from severe eccentric damage or high-volume hypertrophy sessions, daily application for 5–7 consecutive days provides sustained mitochondrial support throughout the repair timeline.
Key takeaway: Therapeutic efficacy depends on precise dosimetry—energy density, irradiance, timing, and spectral purity must all fall within established parameters to achieve the biphasic sweet spot for repair acceleration.
Integrating 670nm Therapy Within a Comprehensive Recovery Architecture
We position 670nm red light therapy not as an isolated intervention but as one component within a systematized recovery architecture. Its mechanisms—mitochondrial energization, inflammatory modulation, collagen upregulation, and perfusion enhancement—complement but do not replace the foundational requirements of protein availability, sleep-mediated growth hormone pulsatility, mechanical unloading periodization, and progressive overload management.
What 670nm therapy offers uniquely is a non-pharmacological, non-invasive modality that directly interfaces with the bioenergetic machinery of repair at the organelle level. No nutritional intervention acts on cytochrome c oxidase with this specificity. No passive rest protocol stimulates fibroblast collagen synthesis at this rate. The wavelength fills a mechanistic gap in the recovery timeline that other modalities cannot address with equivalent precision.
We continue to monitor emerging research—particularly trials isolating the 670nm wavelength from broader spectral bands—and will update our protocols as evidence matures. The current body of literature, while graded conservatively in systematic reviews, demonstrates sufficient mechanistic coherence and directional consistency to justify clinical integration for athletes and trainees pursuing optimized muscle tissue repair outcomes.
1 thought on “How 670nm Red Light Therapy Accelerates Muscle Tissue Repair”
Comments are closed.